
Our Health Library information does not replace the advice of a doctor. Please be advised that this information is made available to assist our patients to learn more about their health. Our providers may not see and/or treat all topics found herein. Childhood Hodgkin lymphoma is a cancer that develops in the lymph system. The lymph system is part of the immune system. It helps protect the body from infection and disease. The lymph system is made up of the following: Bits of lymph tissue are also found in other parts of the body such as the lining of the gastrointestinal tract, bronchus, and skin. There are two general types of lymphoma: Hodgkin lymphoma and non-Hodgkin lymphoma. This summary is about the treatment of childhood Hodgkin lymphoma. Hodgkin lymphoma occurs most often in adolescents 15 to 19 years of age. The treatment for children and adolescents is different than treatment for adults. Other PDQ summaries with information related to lymphoma include the following: The two main types of childhood Hodgkin lymphoma are classic and nodular lymphocyte-predominant. Classic Hodgkin lymphoma is divided into four subtypes, based on how the cancer cells look under a microscope: Epstein-Barr virus infection and a family history of Hodgkin lymphoma can increase the risk of childhood Hodgkin lymphoma. Anything that increases a person's chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop childhood Hodgkin lymphoma, and it can develop in some children who don't have any known risk factors. Talk with your child's doctor if you think your child may be at risk. Risk factors for childhood Hodgkin lymphoma include the following: Inherited changes in genes may increase the risk of childhood Hodgkin lymphoma. Being exposed to common infections in early childhood may decrease the risk of Hodgkin lymphoma in children. Signs of childhood Hodgkin lymphoma include swollen lymph nodes, fever, drenching night sweats, and weight loss. The signs and symptoms of Hodgkin lymphoma depend on where the cancer forms in the body and the size of the cancer. It's important to check with your child's doctor if your child has any symptoms below: Fever for no known reason, weight loss for no known reason, or drenching night sweats are called B symptoms. B symptoms are an important part of staging Hodgkin lymphoma and understanding the patient's chance of recovery. These symptoms may be caused by conditions other than childhood Hodgkin lymphoma. The only way to know is to see your child's doctor. The doctor will ask you when the symptoms started and how often your child has been having them as a first step in making a diagnosis. Tests that examine the lymph system and other parts of the body are used to diagnose and stage childhood Hodgkin lymphoma. If your child has symptoms that suggest Hodgkin lymphoma, their doctor will need to find out if these are due to cancer or to another condition. They will ask about your child's personal and family health history and do a physical exam. The doctor may recommend diagnostic tests to find out if your child has Hodgkin lymphoma. The results of these tests will also help you and your child's doctor plan treatment. The following tests and procedures may be used: A pathologist views the lymph node tissue under a microscope to check for cancer cells called Reed-Sternberg cells. Reed-Sternberg cells are common in classic Hodgkin lymphoma. The following test may be done on tissue that was removed: You may want to get a second opinion. You may want to get a second opinion to confirm your child's diagnosis and treatment plan. If you seek a second opinion, you will need to get important medical test results from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans before giving a recommendation. They may agree with the first doctor, suggest changes or another approach, or provide more information about your child's cancer. To learn more about choosing a doctor and getting a second opinion, see Finding Cancer Care. You can contact NCI's Cancer Information Service via chat, email, or phone (both in English and Spanish) for help finding a doctor or hospital that can provide a second opinion. For questions you might want to ask at your appointments, see Questions to Ask Your Doctor. Certain factors affect prognosis (chance of recovery) and treatment options. If your child has been diagnosed with Hodgkin lymphoma, you may have questions about how serious the cancer is and your child's chances of survival. The likely outcome or course of a disease is called prognosis. The prognosis and treatment options depend on the following: The treatment options also depend on: Most children and adolescents with newly diagnosed Hodgkin lymphoma can be cured. Your child's cancer care team is in the best position to talk with you about your child's prognosis. After childhood Hodgkin lymphoma has been diagnosed, tests are done to find out if cancer cells have spread within the lymph system or to other parts of the body. The process used to find out if cancer has spread is called staging. The information gathered from the staging process determines the stage of the disease. The results of the tests and procedures done to diagnose and stage Hodgkin lymphoma are used to help make decisions about treatment. There are three ways that cancer spreads in the body. Cancer can spread through tissue, the lymph system, and the blood: The following stages are used for childhood Hodgkin lymphoma: Stage I Stage I is divided into stage I and stage IE. Stage II Stage II is divided into stage II and stage IIE. Stage III In stage III, the cancer is found: Stage IV In stage IV, the cancer: In addition to the stage number, the letters A, B, E, or S may be noted. The letters A, B, E, or S may be used to further describe the stage of childhood Hodgkin lymphoma. Childhood Hodgkin lymphoma is treated according to risk groups. Untreated childhood Hodgkin lymphoma is divided into risk groups based on the stage, size of the tumor, and whether the patient has B symptoms (fever, weight loss, or drenching night sweats). The risk group describes the likelihood that Hodgkin lymphoma will not respond to treatment or recur (come back) after treatment. It is used to plan initial treatment. Low-risk Hodgkin lymphoma requires fewer cycles of treatment, fewer anticancer drugs, and lower doses of anticancer drugs than high-risk lymphoma. Sometimes childhood Hodgkin lymphoma does not respond to treatment or comes back after treatment. Primary refractory Hodgkin lymphoma is cancer that does not respond to initial treatment. Recurrent Hodgkin lymphoma is cancer that has recurred (come back) after it has been treated. The lymphoma may come back in the lymph system or in other parts of the body, such as the lungs, liver, bones, or bone marrow. There are different types of treatment for children with Hodgkin lymphoma. There are different types of treatment for children with Hodgkin lymphoma. You and your child's care team will work together to decide treatment. Many factors will be considered, such as your child's overall health, and whether the tumor is newly diagnosed or has come back. Children with Hodgkin lymphoma should have their treatment planned by a team of health care providers who are experts in treating childhood cancer. A pediatric oncologist, a doctor who specializes in treating children with cancer, will oversee treatment of childhood Hodgkin lymphoma. The pediatric oncologist works with other pediatric health care providers who are experts in treating children with Hodgkin lymphoma and who specialize in certain areas of medicine. These may include the following specialists and others: The treatment of Hodgkin lymphoma in adolescents and young adults may be different than the treatment for children. Some adolescents and young adults are treated with an adult treatment regimen. The following types of treatment may be used: Chemotherapy Chemotherapy is a cancer treatment that uses one or more drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. Cancer treatment using more than one chemotherapy drug is called combination chemotherapy. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). The way the chemotherapy is given depends on the risk group. For example, children with low-risk Hodgkin lymphoma receive fewer cycles of treatment, fewer anticancer drugs, and lower doses of anticancer drugs than children with high-risk lymphoma. For more information, see Drugs Approved for Hodgkin Lymphoma. Radiation therapy Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. These types of external radiation therapy include the following: Radiation therapy may be given, based on the child's risk group and chemotherapy regimen. The radiation is given only to the lymph nodes or other areas with cancer. Targeted therapy Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Types of targeted therapy include the following: Rituximab or brentuximab may be used to treat high-risk, refractory, or recurrent childhood Hodgkin lymphoma. Bortezomib is a proteasome inhibitor used to treat refractory or recurrent childhood Hodgkin lymphoma. To learn more, see Targeted Therapy to Treat Cancer. Immunotherapy Immunotherapy uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. Types of immunotherapy include the following: Pembrolizumab and nivolumab are types of PD-1 inhibitors that may be used in the treatment of childhood Hodgkin lymphoma that has come back after treatment. Nivolumab is being studied to treat high-risk childhood Hodgkin lymphoma. Surgery Surgery may be done to remove as much of the tumor as possible for localized nodular lymphocyte-predominant Hodgkin lymphoma in children. High-dose chemotherapy with stem cell transplant High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells. For more information, see Drugs Approved for Hodgkin Lymphoma. Clinical trials A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. Because cancer in children is rare, taking part in a clinical trial should be considered. Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. Some clinical trials are open only to patients who have not started treatment. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website. To learn more, see Clinical Trials Information for Patients and Caregivers. Proton beam radiation therapy Proton-beam therapy is a type of high-energy, external radiation therapy that uses streams of protons (small, positively-charged particles of matter) to make radiation. This type of radiation therapy may help lessen the damage to healthy tissue near the tumor, such as the breast, heart, and lungs. Treatment for childhood Hodgkin lymphoma causes side effects and late effects. To learn more about side effects that begin during treatment for cancer, visit Side Effects. Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Because late effects affect health and development, regular follow-up exams are important. Late effects of cancer treatment may include the following: For female survivors of Hodgkin lymphoma, there is an increased risk of breast cancer. This risk depends on the amount of radiation the breast received during treatment and the chemotherapy regimen used. The risk of breast cancer is decreased if radiation to the ovaries was also given. It is suggested that female survivors who received radiation therapy to the breast have a mammogram and MRI once a year starting 8 years after treatment or at age 25 years, whichever is later. It is also suggested that female survivors do a breast self-exam every month beginning at puberty and have a breast exam done by a health professional every year beginning at puberty until age 25 years. The breast exams done by a health professional will increase to every 6 months at age 25 years. For male survivors who received radiation therapy to the chest, there may be a higher risk of cardiovascular disease. Limiting radiation therapy to the chest is suggested if possible. Some late effects may be treated or controlled. It is important to talk with your child's doctors about the possible late effects caused by some treatments. To learn more, see Late Effects of Treatment for Childhood Cancer. Patients may want to think about taking part in a clinical trial. For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment. Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment. Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward. Patients can enter clinical trials before, during, or after starting their cancer treatment. Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment. Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website. Follow-up tests may be needed. As your child goes through treatment, they will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests. Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back). For patients who receive chemotherapy alone, a PET scan may be done 3 weeks or more after treatment ends. For patients who receive radiation therapy last, a PET scan should not be done until 8 to 12 weeks after treatment ends. This information does not replace the advice of a doctor. Ignite Healthwise, LLC disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use and Privacy Policy. Learn how we develop our content. Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.Childhood Hodgkin Lymphoma Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Childhood Hodgkin Lymphoma

The lymph system is part of the body's immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph (clear, watery fluid) and lymphocytes (white blood cells) travel through the lymph vessels and into the lymph nodes where the lymphocytes destroy harmful substances. The lymph enters the bloodstream through a large vein near the heart.
Reed-Sternberg cell. Reed-Sternberg cells are large, abnormal lymphocytes (a type of white blood cell) that may contain more than one nucleus. These cells are found in people with Hodgkin lymphoma. Reed-Sternberg cells are also called Hodgkin and Reed-Sternberg cells.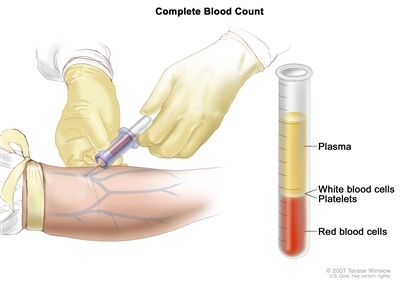
Complete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions.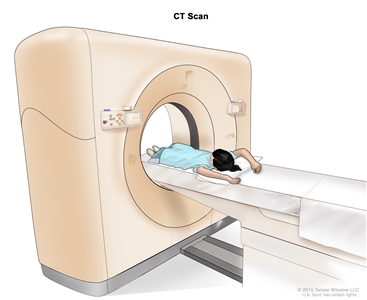
Computed tomography (CT) scan. The child lies on a table that slides through the CT scanner, which takes a series of detailed x-ray pictures of areas inside the body.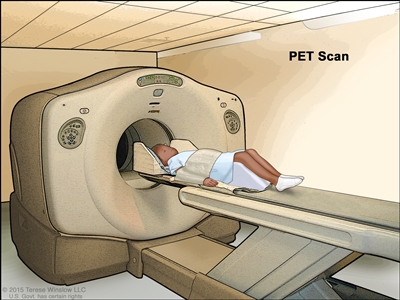
Positron emission tomography (PET) scan. The child lies on a table that slides through the PET scanner. The head rest and white strap help the child lie still. A small amount of radioactive glucose (sugar) is injected into the child's vein, and a scanner makes a picture of where the glucose is being used in the body. Cancer cells show up brighter in the picture because they take up more glucose than normal cells do. 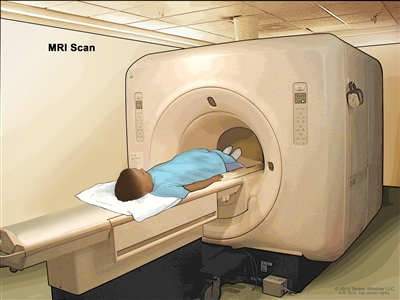
Magnetic resonance imaging (MRI) scan. The child lies on a table that slides into the MRI machine, which takes a series of detailed pictures of areas inside the body. The positioning of the child on the table depends on the part of the body being imaged.
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the child's hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope.Stages of Childhood Hodgkin Lymphoma

Stage I childhood Hodgkin lymphoma. Cancer is found in one or more lymph nodes in a group of lymph nodes or, in rare cases, cancer is found in the Waldeyer's ring, thymus, or spleen. In stage IE (not shown), cancer has spread to one area outside the lymph system.
Stage II childhood Hodgkin lymphoma. Cancer is found in two or more lymph node groups that are either above the diaphragm or below the diaphragm.
Stage IIE childhood Hodgkin lymphoma. Cancer has spread from a group of lymph nodes to a nearby organ or area that is outside the lymph system.
Stage III childhood Hodgkin lymphoma. Cancer is found (a) in lymph node groups above and below the diaphragm; or (b) in lymph node groups above the diaphragm and in the spleen.
Stage IV childhood Hodgkin lymphoma. Cancer (a) has spread throughout one or more organs outside the lymph system, such as the liver; or (b) is found in two or more groups of lymph nodes that are on the same side of the diaphragm and in an organ that is outside the lymph system, such as the lung, and not near the affected lymph nodes; or (c) is found in groups of lymph nodes on both sides of the diaphragm and in any organ that is outside the lymph system, such as the lung; or (d) has spread to the lungs, liver, or bone marrow from areas far away.Treatment Option Overview
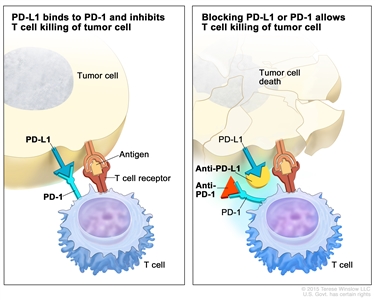
Immune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel). immune checkpoint inhibitorsImmunotherapy uses the body's immune system to fight cancer. This animation explains one type of immunotherapy that uses immune checkpoint inhibitors to treat cancer.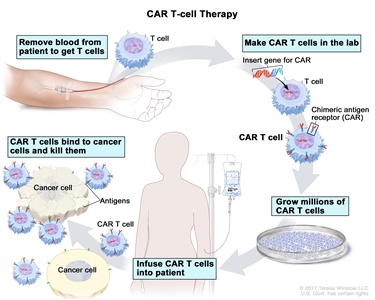
CAR T-cell therapy. A type of treatment in which a patient's T cells (a type of immune cell) are changed in the laboratory so they will bind to cancer cells and kill them. Blood from a vein in the patient's arm flows through a tube to an apheresis machine (not shown), which removes the white blood cells, including the T cells, and sends the rest of the blood back to the patient. Then, the gene for a special receptor called a chimeric antigen receptor (CAR) is inserted into the T cells in the laboratory. Millions of the CAR T cells are grown in the laboratory and then given to the patient by infusion. The CAR T cells are able to bind to an antigen on the cancer cells and kill them.

Patient Education